Colon polyps are growths that form in the lining of the large intestine, and while most are harmless, some can pose serious health risks. These protrusions of the mucous membrane are common, especially as we age, but their potential to develop into colon cancer makes awareness and prevention critical. In this article, we’ll explore what colon polyps are, their types, how they’re detected, and steps you can take to reduce your risk—drawing from medical expertise and practical experience.
What are Colon polyps?
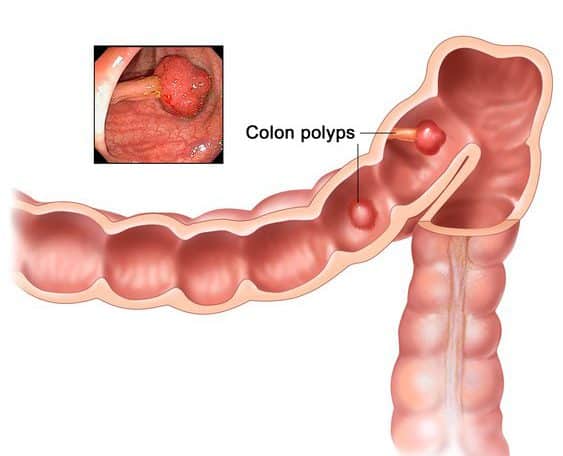
Colon polyps are abnormal tissue growths that protrude from the intestinal mucosa into the colon’s interior, known as the intestinal lumen. They typically form in the large intestine, especially the rectum, due to an overgrowth of cells in the mucous membrane. While many people have colon polyps—particularly as they age—most remain benign. However, certain types can evolve into colon cancer over years, making early detection vital.
Most colon polyps don’t cause symptoms, which is why they’re often found during routine screenings like colonoscopies. A tiny polyp bud can grow over time, and in some cases, its tissue may become malignant, leading to uncontrolled cell growth—colon cancer. Factors like age, genetics, and lifestyle influence their development.
What are intestinal polyps? Are they dangerous?
Many people have polyps in their intestines. The older you get, the more common they occur. Intestinal polyps are protrusions of the mucous membrane that protrude from the intestinal mucosa into the inside of the intestine – the intestinal lumen. They arise because more cells than normal grow in one or more places in the mucous membrane. The polyps are typically found in the large intestine, especially in the last section, the rectum.
Most colon polyps are benign, so colon cancer will not develop from them. However, some polyps can develop into colon cancer over the course of years. Initially, a tiny polyp forms – a polyp bud. This can increase over time. For various reasons, the polyp tissue can become malignant, usually over a period of many years. The cells in the tissue grow in an uncontrolled manner. This is known as colon cancer.
How cancer can develop from polyps
The progression from a polyp to cancer begins with a small tissue growth that enlarges over time. For reasons such as genetic mutations or chronic inflammation, the polyp can turn malignant. The resulting tumor may invade the colon’s muscle layer, spreading through blood or lymph vessels to form metastases elsewhere in the body. If undetected, a tumor can block the intestine or breach the intestinal wall, affecting nearby organs. This slow process underscores the importance of regular screening.
Types of Colon Polyps
Colon polyps vary in shape, structure, and risk level. Here’s a breakdown based on microscopic analysis after removal:
Hyperplastic Polyps: Usually benign, these sit flat on the mucosa with a sawtooth appearance.
Inflammatory Polyps: Linked to conditions like Crohn’s disease or ulcerative colitis, they rarely become cancerous.
Adenomas: The most common potentially harmful type, adenomas (or adenomatous polyps) include tubular, villous, and tubulovillous forms. Over 90% of colon cancers arise from adenomas, especially larger ones or those in hereditary conditions like familial adenomatous polyposis (FAP).
Harmful Polyps: Seen in hereditary syndromes, these can affect children and carry a high cancer risk.
Adenomas are a key focus in cancer prevention, as their removal during colonoscopy significantly reduces risk.
Risk Factors for Colon Polyps
Several factors increase the likelihood of developing colon polyps:
Age: Risk rises after 50.
Obesity: Higher body mass index correlates with polyp formation.
Lifestyle: Low fiber intake, frequent red meat consumption, smoking, and alcohol use contribute.
Inflammation: Diets high in sugar, trans fats, or processed foods may play a role.
Genetics: Conditions like FAP or Lynch syndrome heighten risk, often with a family history of colon cancer.
Gender: Men are slightly more prone than women.
Symptoms and Detection
Colon polyps rarely cause noticeable symptoms. Occasionally, larger polyps may bleed (visible as blood in the stool) or disrupt digestion, leading to constipation or diarrhea. The gold standard for detection is a colonoscopy, where a gastroenterologist uses an endoscope to examine the colon, identify polyps, and remove them for biopsy. Stool tests for occult blood are an alternative but less reliable, as not all polyps bleed.
For those over 50, Medicare often covers colonoscopies if a stool test is positive, typically offered every 5 years, with higher-risk individuals screened earlier.
Treatment and Follow-Up
Polyps are removed during colonoscopy using tools like a snare or forceps, then analyzed to determine if they’re benign or malignant. Post-removal, follow-up colonoscopies are scheduled based on risk—often every 3-5 years for those with adenomas. To support colon health, experts suggest a fiber-rich diet, hydration (3 liters of water daily), and supplements like omega-3s, vitamin C, and probiotics. Taking a psyllium-based product like AIM Herbal Fiberblend to gently and regularly clean the colon is most helpful.
If you feel that you have some inflammation going on try our ‘natural penicillin’ recipe.
Preventing Colon Polyps
Reducing your risk of colon polyps aligns with colon cancer prevention strategies:
Stay Active: Aim for 30-60 minutes of exercise daily.
Eat Well: Prioritize vegetables, fruits, whole grains, and legumes; limit red or processed meats.
Avoid Toxins: Cut back on alcohol and quit smoking.
Maintain Weight: Keep a healthy BMI.
Cleanse Regularly: Consider colonics or fiber supplements like psyllium for gut health.
Colon polyps are common but manageable with the right knowledge and care. While most won’t become cancerous, their potential risk warrants proactive steps—regular screenings, a healthy lifestyle, and awareness of your family history. Consult a healthcare provider for personalized advice, especially if you’re over 50 or have risk factors.
Colonics are a great way to help keep your colon clean and support you in keeping up with a healthy lifestyle.
With Restless Leg Syndrome there is an agonizing feeling of restlessness and the urge to move the legs, especially in the evening and at night.
In a nutshell: What is Restless Legs Syndrome?
Restless legs syndrome (RLS, restless legs, Wittmaack-Ekbom syndrome) causes excruciating restlessness and tension in the legs, possibly also tingling, pulling or stinging. The arms are less often affected. The unpleasant sensations occur almost exclusively at rest, especially in the evening and at night, and rob you of sleep. Movement brings only short-term improvement.
Restless legs occur during pregnancy. The symptoms usually go away after birth.
If the restless legs are due to another disease than they will mostly resolve once the disease is taken care of. Otherwise, CBD oil is helpful or as a last resort, medication will help if the symptoms are severe.
Experts estimate that RLS affects around 5 to 10 percent of the population. The risk increases with age. There is a family form. Here the disease may already be noticeable before the age of 30. In rare cases, restless legs appear in children. The symptoms can then be mistaken for growing pains or attention deficit hyperactivity disorder (ADHD).
What are the typical symptoms of RLS?
It is not always easy for those affected to describe their symptoms. Symptoms can vary from patient to patient. Nevertheless, there are distinctive features:
Those affected feel an uncomfortable feeling of tension and restlessness in the legs, and less often in the arms. Some patients also describe tingling, tearing, or stinging
They have an insatiable need to move, to tense or stretch their leg muscles
The unbearable restlessness occurs especially in the evening and at night, when those affected actually want to rest or sleep
The symptoms improve temporarily through activity – for example when the sick stand up and walk around. Some people give their legs a cold shower or massage. Afterwards, however, the complaints often return immediately
The restlessness in the legs makes it difficult for those affected to fall asleep, often not sleeping through the night, and they are tired and exhausted during the day
Restless legs syndrome can severely restrict everyday life. Sitting for long periods – for example in the cinema, on the plane or in a restaurant – becomes torture. Friends and family do not always understand.
Causes: How does Restless Legs Syndrome develop?
Restless legs probably arise because the transmission of messages in the nervous system is disrupted. The exact causes have not yet been clarified.
Researchers assume that restless legs are partly inherited, as the syndrome often affects several family members (familial RLS). If parents or siblings are ill, your own risk increases. In addition, certain changes in the genetic makeup (genes) increase the likelihood of developing restless legs.
Restless legs can occur due to external influences or accompanying them (secondary RLS):
Iron deficiency
Kidney dysfunction
Pregnancy
Neurological diseases such as polyneuropathy or Parkinson ‘s disease
Some medications can trigger or worsen Restless Legs Syndrome.
How do you diagnose RLS?
If RLS also occurs in family members, this makes the diagnosis more likely. The following four points speak in favor of restless legs syndrome:
Those affected feel an uncomfortable urge to move, mostly in the legs, possibly associated with sensory disturbances or pain
Symptoms mainly occur at rest
Exercise temporarily relieves symptoms
The symptoms are particularly noticeable in the evening and at night
A neurological examination sometimes also provides indications of an (accompanying) nerve disease.
Restless legs syndrome can be the result of other diseases or disorders. To find them, your practitioner can do additional tests:
A blood test can rule out an iron deficiency. The ferritin value should be in the upper normal range
The kidney values in the blood provide information about the kidney function
The thyroid values can reveal thyroid disorders
Symptoms of RLS sometimes resemble those of the nerve disorder polyneuropathy. In order to delimit them, a doctor can measure the nerve conduction speed (electroneurography) and the functioning of the muscles (electromyography).
If sleep disorders and pronounced daytime sleepiness are in the foreground, an examination in the sleep laboratory can be informative. The doctors use special measuring devices to record involuntary leg movements during sleep, for example. In this way, other causes of disturbed sleep can be identified.
L-dopa test
The L-Dopa test can confirm the suspicion of restless legs. The drug L-Dopa turns into dopamine in the brain. This influences the signal transmission of the nerves. In the L-Dopa test, the patient receives L-Dopa as soon as the symptoms set in. If the symptoms improve, this indicates a high probability of restless legs syndrome. However, if there is no improvement, this does not speak against RLS.
Therapy: what helps with Restless Legs Syndrome?
Whether restless legs syndrome should be treated is always an individual decision.
RLS can occur during pregnancy. Then it often disappears after delivery.
If the syndrome developed due to a disease or disorder, sometimes treating it is enough:
In the case of iron deficiency, the patient is given iron as a preparation or infusion
Severe renal impairment must be treated appropriately
Some medications can make restless legs syndrome worse. It may be possible – in consultation with the doctor – to swap the drugs for more suitable ones.
Therapy with drugs
If the cause of Restless Legs Syndrome is unknown, symptoms can be treated with medication. The syndrome itself is currently incurable.
Many people affected are helped by active ingredients that are also used in higher doses against Parkinson’s disease, such as dopamine preparations. Similar to the body’s own messenger substance dopamine, these drugs act on the communication between nerve cells. With all of these drugs, side effects such as nausea or dizziness can occur, especially in the first time after starting therapy.
In addition to the Parkinson’s medication, an opiate (oxycodone and naloxone) is approved for severe RLS, which is slowly released into the bloodstream after ingestion (retarded).
“Augmentation” problem
Sometimes dopamine supplements exacerbate the symptoms of Restless Legs Syndrome, which is medically called augmentation. The risk of augmentation increases the higher the dose of Parkinson’s medication. The symptoms develop earlier in the day and not in the evening or at night. Often they are more agonizing than before. They set in more quickly when they are at rest and can spread to other parts of the body. Augmentation can be treated by switching to another drug.
What else can help?
Some patients have good experiences with home remedies such as alternating showers or light gymnastics. Some try homeopathy. It is unclear whether magnesium supplements will help. Some patients have good results with CBD oil.
Restless legs syndrome can severely impair the quality of life and psychological well-being. In such cases, the possibility of psychotherapeutic support should be considered. The exchange with other affected persons – for example in a self-help group – may have relief.
It is unlikely that colonics will help with restless legs as such, and we don’t know yet if our microbiome can help with this problem. But seeing that about 50% dopamine is produced in the gastrointestinal tract by enteric neurons and intestinal epithelial cells, it makes sense that it is important to keep it well functioning.
The body often needs nutritional support in recovery. With the right food, you can help get back on your feet after an illness.
Illness comes – appetite goes. This is a big problem, especially in old age. But not eating anything is not the solution.
Whereas in the past diets were prescribed for diseases of the stomach and intestines, the following applies today: What tastes good and what is tolerated is allowed.
The shorter a meal stays in the stomach, the more digestible we find it. Chew well, because liquids and pulps pass the stomach quickly.
Steamed food is easier to digest than fried food, rice with vegetables is more digestible than a piece of fatty meat. Be careful with hot spices such as pepper, curry or paprika!
Do not burden the stomach with large meals, rather eat small portions more often. And last but not least: Try to calm down – with stress or anger in your stomach, the best food becomes a burden. We Have all heard this advice over and over again. It is reinforced by doctors internationally, yet so many people suffer from poor nutrition?
Nutrition is no big secret. Soups are great for nutrition because of all the nutrients they contain, with or without protein. They are also very easy for the body to digest and thus offer better absorption of those valuable nutrients.
1. Something warm
Hot chicken soup has a tradition as food for the sick. I have a Polish friend that calls chicken soup ‘Jewish Penicillin.’ The steam that moistens the mucous membranes when sipping, the hot liquid in general, minerals such as zinc, the anti-inflammatory substances in the bones, or the care of the cook: various factors probably play a role in the beneficial effect. It just shows that the now so popular ‘Bone Broth’ is really nothing new.
Tip: leave some meat in the soup, it contains well-tolerated protein, vegetables contain additional minerals. The soup becomes even more substantial with gluten-free noodles.
2. Start easily
An infection is often associated with involuntary fasting. After the break, you should start again as soon as possible, but especially after a gastrointestinal infection, do not put too much pressure on your digestion. Ideal starters are rusks, toast or a porridge made from oatmeal and water. Tip: expand the menu as soon as possible, otherwise the diet will become too one-sided in the long run! Oatmeal can be gradually “built-up”: with any kind of milk, banana or other fruits, nuts or almonds.
3. Fill up with water
No thirst and at the same time fever, vomiting or diarrhea means the body quickly lacks fluids. Drinking is important so that the circulation does not sag, the brain and organs receive sufficient nutrients and because the kidneys can only excrete toxins in water. Hot drinks are particularly beneficial.
Instead of black tea and coffee, choose herbal teas with additional effects: chamomile, lemon balm, peppermint soothe the stomach, caraway seeds and fennel relieve flatulence. Icelandic moss is good for sore throats, thyme loosens phlegm, and linden flowers help with coughs.
4. Refuel with something fresh
In order to work properly, the immune system needs enough vitamins and minerals. Lots of vegetables and fruit provide a healthy basis for this. In addition, the green diet helps to stabilize the balance of the intestinal bacteria, which are important for the immune system. Carrots and zucchini are easier to digest than cabbage and leeks, and cooked vegetables are easier to digest than raw vegetables. Additional calories in the form of butter or oil are now desirable.
5. Invigorate the intestines
If you have to take Antibiotics, they relieve symptoms quickly, but about one in four gets diarrhea from them. Yoghurt cannot prevent this with certainty, but it can help. Experts suspect that the yoghurt bacteria displace the pathogenic germs in the intestine. The correct dose is two to three cups a day. If you can’t eat that much yoghurt, take a good multistrain probiotic.
Important: The effect of some antibiotics is inhibited by dairy products. Eat yogurt or probiotics as far away from the antibiotics as possible (4hrs).
6. Lots of protein
Muscles that atrophy easily when lying down need a lot of protein in addition to movement. Eggs are a good source. It is even more valuable when combined with potatoes, for example as frittata: protein building blocks that one lacks is provided by the other and vice versa.
Spread the protein sources over the day: Start in the morning with cheese and bread or porridge with milk. Eat scrambled eggs, steamed fish or a steak at lunchtime and a sausage sandwich or a glass of milk as a bedtime treat in the evening. Vegetarians are right with lentils etc – ideal with bread or pasta.
Colon Hydrotherapy or an enema is always helpful during recovery from anything. Simply because it supports our immune system, which in turn supports our healing.
Iridology, Eyology and Sclerology are similar but slightly different practices all of which involve the observation of the markings and colourings in the anterior layers of the eye. It is believed that through the identification of this differences, direct relationships with illness or malady in the body can be diagnosed.
In addition to illness many other health factors can be determined about the patient which include, genetic predisposition, inherited traits, organ functionality and general health and well being. With this knowledge a protocol can be recommended by the practitioner for healing.
With an anal fissure, the sensitive skin in the anal canal tears and an ulcer forms. The reasons behind this have not yet been clarified. Factors such as constipation with heavy straining during bowel movements, but also hemorrhoids or diarrhea seem to increase the risk of anal canal ulcer. An anal fissure can also occur in the context of certain underlying diseases such as Crohn’s disease. Women in menopause can also be affected due to increased dryness in this area (Lichen Sclerosus).
The tear usually causes severe, sometimes burning pain when defecating. In addition, there is often bright red blood in the stool or on the toilet paper. Symptoms such as itching or burning can also indicate an anal fissure.
The therapy of the actual anal fissure is to keep the stool soft. Ointments and suppositories are used as support. The acute anal fissure usually heals with time. If you suffer from a chronic anal fissure, the only remaining option is surgical treatment.
What is an anal fissure (anal tear)?
Doctors speak of an anal fissure when the very sensitive skin in or near the anal canal (anoderm) tears and an elongated ulcer forms.
Anal fissures can affect people of all ages, men as well as women. Anal cracks occur particularly frequently between the ages of 30 and 40. Doctors differentiate between acute and chronic anal fissures. Some authors recommend dividing the anal fissure into a spastic (= acute) and an inflammatory (= chronic) form according to its mechanism of origin.
While the acute anal fissure usually heals, a chronic anal fissure can show further changes in the anus. So an outpost fold (= mariske) can form. Although this thickening of the skin is largely harmless, it interferes with hygiene. An anal fibroma (a benign connective tissue nodule) as well as scarred, bulging marginal walls around the ulcer or fistulas (duct formation) can also develop.
What are the causes and risk factors of an anal fissure?
If the “session” is painful, this often leads to constipation
Researchers do not yet know what exactly leads to an anus tear. However, the texture of the stool seems to play a major role in whether an anal fissure occurs. For example, those who suffer from constipation, i.e. have a hard bowel movement, are more likely to get painful anal cracks. Strong pressure when defecating also increases the risk of injuring the sensitive inner skin in the anal canal (anoderm). Conversely, diarrhea or mushy stool can also promote anal cracks.
Another risk factor: hemorrhoids. Because the anoderm is already damaged and can tear more easily. Infections – for example, cryptitis (inflammation in the area of the rectum) – reduced blood flow to the anal skin or cramped sphincter muscles in the anus can lead to an anal fissure. Sometimes an anal fissure occurs as a result of an underlying disease (secondary anal fissure), for example in Crohn’s disease.
Symptoms: What are the symptoms of an anal fissure?
An anus tear typically causes stabbing or burning pain when defecating. The pain can go away immediately after a bowel movement, but can also reappear after a short, pain-free interval and last for hours. The tears in the special skin in the anal canal (anoderm) are often noticeable through bright red blood stains on the toilet paper or the chair. In addition, the anus can itch, burn or ooze.
A vicious circle begins, as an anal rupture can cause severe pain, often resulting in restrained bowel movements (constipation). However, the hardened stool irritates the wound and the anal fissure can deepen. This in turn increases the pain. As a result, the sphincter muscles also tighten, which increases the problems with bowel movements. In addition, the anoderm is poorly supplied with blood due to the cramped muscles, and the healing process slows down. It is therefore important to break this mechanism.
If you have complaints in the anal area, you should contact your doctor. They can then refer you to a specialist in rectal diseases (proctologist), as there may be a possible anal fissure as well as many different causes of problems in the rectum area (for example hemorrhoids, tumors or ulcers). We therefore urgently recommend clarifying any complaints in the anal area!
Diagnosis: how does the doctor determine an anal fissure?
In addition to the anamnesis, an examination of the external anal area is carried out, whereby the painful tear is partially discovered. Most anal fissures are longitudinal and occur towards the tailbone.
If the external inspection is not sufficient, the anal canal is examined further under local anesthesia, as the examination can otherwise be quite painful.
Anal fissures can be challenging to treat naturally. Keeping the stool soft is most important. Using something like Oxy-Powder works best. Also using emu cream or calendula cream 3x per day and after every bowel motion, usually give good results if the fissure is not spastic or chronic. If the area seems to be infected, Lugols iodine can be dapped onto the fissure.
The therapy of the acute (spastic) fissure aims at lowering the pressure of the sphincter muscle. Furthermore, ointments with nitroglycerin or calcium antagonists are used for topical therapy. Both ointments are to be used three to four times a day for about six to eight weeks. A stretching treatment can also help.
Another measure to lower the pressure of the sphincter muscle is the therapy with botulinum toxin A (botox). This is injected into the sphincter muscle and causes its paralysis, whereby the increased pressure is reduced. Note that this treatment can lead to temporary incontinence.
With the above-mentioned conservative therapy options, the anal fissure heals in over 90 percent of cases. If therapy fails, surgical therapy may be necessary but should be seen as a last resort.
A chronic (inflammatory) fissure must be treated surgically. Various surgical techniques are available for this, which are determined depending on the location, cause and other findings. If there is scarred tissue or an outpost fold, the attending physician removes the skin or anoderm changes as flatly as possible (fissurectomy). A transection of the sphincter muscle (sphincterotomy), which was often used in the past, is no longer recommended by experts due to the risk of incontinence.
Cracks in the anus are often caused by hard stool and constipation, or when patients strain too hard when defecating. However, you should only use laxatives in exceptional cases. When used frequently, they disrupt the natural regulation of digestion and remove important minerals from the body.
Better: eat enough fiber. Dietary fiber increases the volume of the intestinal contents and thus stimulates digestion. This prevents people from becoming constipated. In addition, fiber makes you full longer and therefore helps to maintain weight. Healthy ingredients can be found in fruits, vegetables and whole-grain products.
Drinking enough fluids (water, unsweetened tea) and exercise are also important. A fluid intake of 1.5 litres should be achieved – provided there are no underlying diseases such as impaired kidney function to prevent it. More exercise can often be built into everyday life: take a regular walk, cycle to the bakery or go for a walk.
References:
– Classen, Diehl, Kochsiek: Internal Medicine, Elsevier, Urban & Fischer, 6th edition – R. Winkler with a contribution by WH Jost, pp. 143-158 “Anal fissure” from J. Lange et al.: “Chirurgische Proktologie”, Springer Verlag, 2012 – Raulf F., Kolbert GW: Practical Handbook Coloproctology Dr. Kade (2006) – G. Kolbert, M. Stoll: Guideline-compliant therapy of anal fissures, coloproctology 5/2016 – H. Mlitz, V. Wienert, F. Raulf, Analfissur, self-published, 2012
Anal Fissures are contraindicative for Colonics, but there are other ways to clean your colon even with Anal fissures.
Pain in the abdomen can have a variety of causes – depending on whether they are acute or chronic, in women or men
For many people, abdominal pain is still synonymous with women’s ailments, i.e. complaints that primarily affect the female genital organs. Pain in the lower third of the abdominal region, i.e. in the lower abdomen, is not just a woman’s concern. Men can also experience abdominal pain.
First and foremost, it is about the organs in the lower pelvic space, including the small pelvis. These are the (internal) genital organs, the urinary bladder with the urethra and the ureters that open at the sides, the appendix and the lower intestinal parts, vessels, nerves and lymph nodes.
Abdominal pain in women: Often before and during your period
Typical abdominal pain includes period pain that many women feel before and during their period: as pulling in the abdomen or in the lower back or as cramp-like pain. They are individually very different, mostly not pathological and change many times, depending on the life situation and phase.
Some women also experience drawing pains for a day or two between menstrual bleeds, often on one side or over the pubic hair area. This middle pain often marks ovulation. Even if there are no other symptoms, it is advisable to speak to your gynecologist about such pain to make sure that no other problems are the cause. Because acute or chronic complaints can conceal, for example, inflammations and diseases of the genital organs or the urinary tract.
If a woman starts to have spotting and abdominal pain, especially if she did not have periods before, the gynecologist will conduct targeted examinations to check whether there is an ectopic pregnancy.
In the case of abdominal pain during pregnancy, greater caution should be exercised if something changes in the abdomen. The complaints in expectant mothers can have special reasons, harmless but also alarming, which the gynecologist will clarify immediately. This article does not deal with this.
In men and women: Acute abdominal pain …
Discomfort in the lower abdomen can be acute. They then either indicate a temporary, rather harmless disorder or they represent alarm signals that a practitioner should investigate immediately. This is especially true if they are very violent and there are also symptoms such as fever, nausea, indigestion such as diarrhea or constipation, pain when emptying the bladder and/or bleeding.
The causes of sudden onset of severe pain are often acute inflammation, such as of the appendix or intestine, fallopian tubes, ovaries or urinary tract. Urinary stones, twisting and breakthroughs in tumours or parts of the intestine can also trigger threatening abdominal pain.
… or: chronic abdominal pain
Doctors speak of chronic pelvic pain if the symptoms persist for six months. They can appear again and again in certain situations or nestle more or less permanently.
There are many causes of chronic pain. Problems are often caused by chronic inflammation and diseases of the genital organs, the urinary tract, the digestive tract, especially the large intestine. Tumor diseases of the individual organs should also be considered. In addition, disorders in the nerves, muscles or spine can be responsible for pelvic pain.
It is not uncommon for psychological problems and illnesses such as depression to be associated with physical symptoms. This can include chronic abdominal pain. On the contrary, possible consequences of the operation such as scarring can only aggravate the pain.
In the case of abdominal pain, a gynecologist or urologist is often the right contact
Lower abdominal pain: when to see a doctor?
Pain in the lower abdomen should always be clarified by a doctor, in particular, if the pain starts suddenly and violently, fever and/or bleeding is added. In addition to the family doctor, the first point of contact is the gynecologist and, for men, the urologist. In addition, a specialist in gastrointestinal diseases (gastroenterologist) is often in demand, possibly also an orthopedist or neurologist.
Abdominal pain: important causes, possible accompanying symptoms
Gynecological diseases, venous diseases
Chlamydia infections (discharge, problems with urination and bowel movements are possible; however, the majority of the infection is chronic and insidious for a long time without causing symptoms)
Inflammation of the uterus (discharge, bleeding outside of the norm)
Inflammation of the fallopian tubes and ovaries (often fever, discharge, intermenstrual bleeding)
Purulent tissue meltdown (abscess)
Rotation of the stem, rupture of cysts on the ovary or tumors (acute pain)
Fibroids, polyps in the uterus (often bleeding disorders)
Endometriosis (often bleeding between periods, severe menstrual pain)
Ectopic pregnancy (no menstruation, followed by abdominal pain, spotting)
Miscarriage, discharge (heavy bleeding)
Cervical cancer, uterine cancer (strong-smelling discharge, bleeding outside of normal periods, after menopause)
Varicose veins, thrombosis of the leg and/or pelvic veins (possible warning signs: in addition to heaviness and pain, swelling in the leg , groin, sensation of warmth, bluish discoloration)
Intestinal disorders, intestinal diseases
constipation
Appendicitis (pain often in the right groin, but also not exactly localizable, diffuse, possibly fever, weakness, nausea, vomiting)