With celiac disease, there is a lifelong intolerance to the adhesive protein gluten. There can be various symptoms depending on the degree of damage to the intestines.
Celiac Disease – In Brief
Patients with celiac disease react to gluten, a protein found in various types of grain. For example, foods containing gluten can cause symptoms such as diarrhea, abdominal pain, or gas. Overall, the symptoms of celiac disease vary widely. Sometimes it goes unnoticed for years. Doctors diagnose celiac disease using blood tests and a small intestine biopsy. Treatment then consists of a lifelong gluten-free diet.
Celiac disease – also called gluten intolerance, indigenous sprue or gluten-sensitive enteropathy – is a disease that has increased in recent years. In the affected people, the ingestion of the gluten contained in various grains leads to inflammation of the small intestine. Gluten is not completely digested in the stomach and upper small intestine. The mucous membrane of the small intestine absorbs the undigested gluten fragments (so-called gluten peptides). Over time, this means that the intestinal mucosa changes and fewer nutrients can be absorbed.
The incidence rates for celiac disease vary from one in 50 to one in 200 people in most countries around the world. In Australia, around every 60th person is affected by celiac disease.
The time of the initial diagnosis is very different. Celiac disease can already be noticed in infants when they start eating complementary foods or only become symptomatic in adulthood – here mostly between the ages of 20 and 60.
What is gluten
Gluten is the predominant protein in grains like wheat, rye, barley, and spelt. For baking, gluten is particularly important because of its dough-forming properties. If the grain is ground into flour and mixed with water, it gets its typical tough mass thanks to the two gluten components gliadin and glutenin. Thanks to their structure, gliadin and glutenin also ensure that bread and pastry dough become loose and rise.
The reason we have such a widespread problem with Gluten is that for the baking industry, grains were changed to contain about 7 times the normal amount of Gluten. This means eating one slice of gluten is like eating 7 slices for your body in regards to Gluten. Our body was just never made to handle that much Gluten.
What happens in the intestine with celiac disease?
The food ingested is broken down into its components in the small intestine. The nutrients are then absorbed through the mucous membrane of the small intestine. If celiac disease is present, the body’s own defense system reacts mistakenly to the gluten fragments, which are also ingested in this way, as to bacteria or other hostile intruders. The lining of the small intestine becomes inflamed. In addition, the body’s defenses are also directed against components of the small intestinal mucosa to which gluten binds.
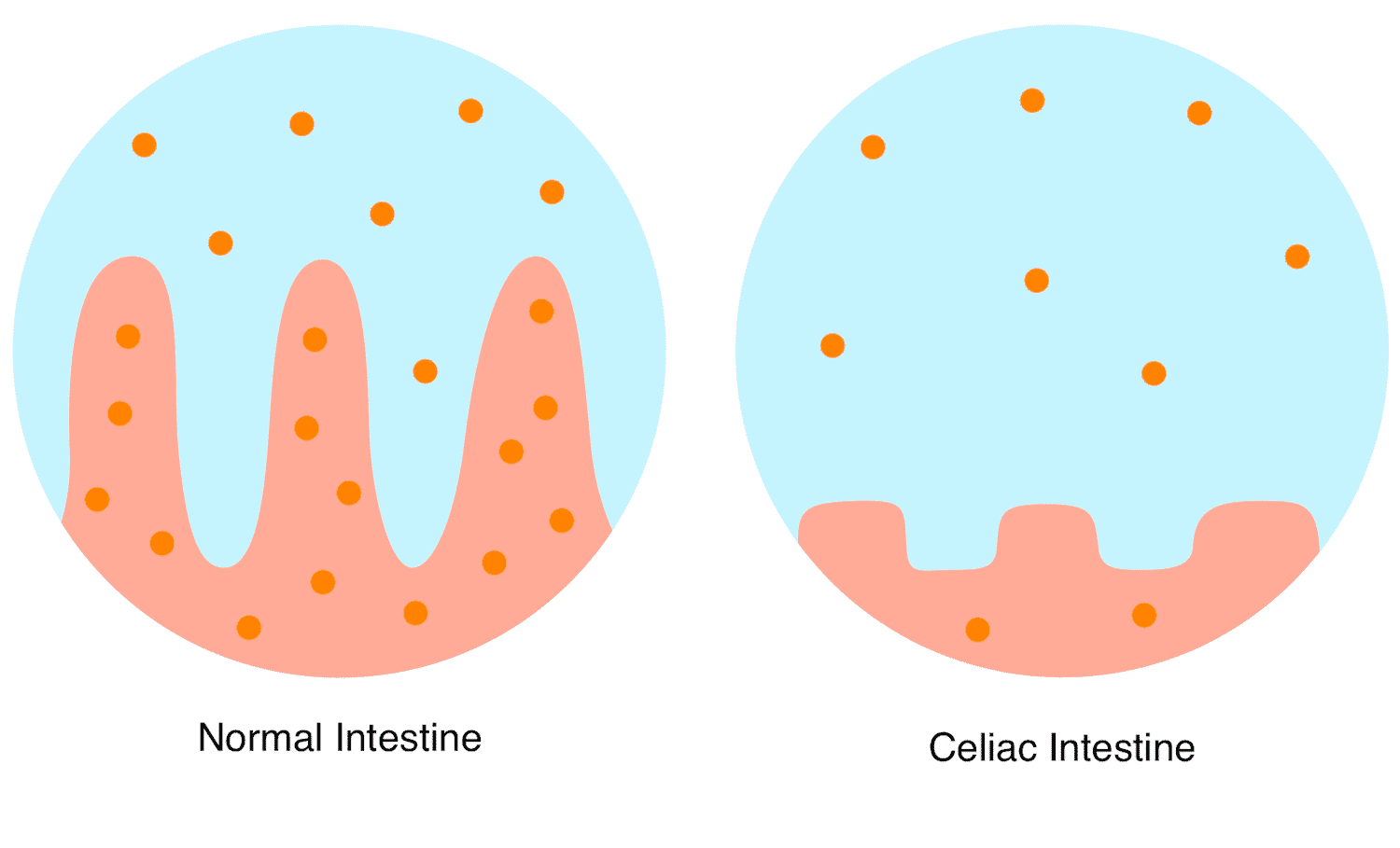
If this inflammation lasts too long because gluten is not avoided, the protrusions of the small intestinal mucosa, the so-called mucous membrane villi, recede over time. This reduces the surface of the intestinal mucosa and fewer nutrients are absorbed from food.
In the event of a severe course, the various food components (e.g. fats, protein, lactose, calcium, iron, vitamins) can only be used insufficiently. Among other things, this can lead to deficiency symptoms such as anemia or bone loss. In addition, children can suffer from developmental disorders such as growth retardation or delayed puberty, and adult women can experience infertility. People who suffer from celiac disease and do not eat gluten-free have an increased risk of developing otherwise rare, malignant small intestinal tumors, adenocarcinoma or the so-called intestinal T-cell lymphoma after years or decades of disease.
Symptoms: What symptoms can celiac disease cause?
Celiac disease is a multi-faceted disease. Doctors therefore also call it a “chameleon of medicine”. The symptoms of celiac disease can be very different.
Some people experience the symptoms badly as soon as they consume even a little gluten.
Others do not notice their illness for years, even though they do not eat a gluten-free diet. Some patients experience typical symptoms such as diarrhea, weight loss, or oily stools.
Others suffer from skin changes (dermatitis herpetiformis Duhring) or recurring canker sores in the mouth.
Others show only indirect signs such as anemia, osteoporosis (bone loss ), infertility or general symptoms such as abdominal pain, fatigue, and joint pain indicate celiac disease.
Deficiency symptoms (for example in vitamin B12, folic acid, vitamin D, calcium or iron ) can also occur.
Adolescents and adults in particular often have hardly any symptoms, although pronounced changes typical of celiac disease can be detected in the mucous membrane of the small intestine. Likewise, there are often only blood values that deviate from the norm, such as inexplicably high liver values. Only when these patients adhere to a gluten-free diet do they notice an improvement in their symptoms.
Classic course most common in babies and toddlers
In babies, the disease is often noticed when the little ones receive cereal products in the form of porridge for the first time. A few weeks to months later, often between six months and one year of age, the classic symptoms of celiac disease can appear:
- Flatulence
- chronic diarrhea
- Large-volume, foul-smelling and shiny stools due to disturbed fat digestion
Other symptoms are:
- Loss of appetite
- Nausea and vomiting
- Weight loss
- Muscle weakness
- Exhaustion
- bulging, distended belly
- bad mood, tearfulness, mental changes
- bad sleep
- Growth and development disorders
However, the symptoms that actually occur vary widely. Sometimes the disease is so inconspicuous that it remains undetected for many years.
Celiac disease often has few symptoms in adolescents and adults
Since celiac disease often only leads to unspecific symptoms in older children, adolescents and adults or even causes no obvious symptoms at all, it is not uncommon for a long time to pass before the disease is recognized. Signs such as abdominal pain, irregular bowel movements or growth retardation in adolescents do not clearly indicate celiac disease. In some cases, the intolerance is only shown indirectly through the consequences of malnutrition. For example; iron deficiency and anemia cause decreased intestinal calcium absorption. In young women, unexplained infertility or frequent miscarriages can indicate celiac disease. In addition, celiac disease must also be considered in the case of certain autoimmune diseases.
In the case of the following diseases and symptoms, the doctor should clarify, among other things, whether celiac disease could also be present:
- Type 1 diabetes mellitus
- Hashimoto’s thyroiditis / hypothyroidism
- Autoimmune hepatitis
- Primary biliary cirrhosis
- Iron deficiency anemia with no other explanation
- Dermatitis herpetiformis Duhring
- Rheumatic diseases
- Recurring canker sores
- Lactose intolerance
- Depressions
- Chronic fatigue
- Unclear increases in liver values
- Osteoporosis
- Osteomalacia
- Irritable bowel syndrome
- Selective IgA deficiency
- Infertility or frequent miscarriages in young women
- Down syndrome
- Turner Syndrome
Forms of Celiac Disease
A distinction is made between the following forms:
Classic celiac disease
Classic celiac disease shows up particularly in toddlers when eating foods containing gluten with the following symptoms:
- distended belly
- voluminous, foul-smelling, greasy diarrhea
- change in behaviour, for example, tearfulness
- failure to thrive and grow
- deficiency symptoms such as iron deficiency
The symptoms disappear quickly with a gluten-free diet.
Symptomatic celiac disease (low)
Symptomatic celiac disease is often much more subtle and is therefore often only discovered late. Sometimes symptoms that have nothing to do with the gastrointestinal tract are also in the foreground. This subtype of symptomatic celiac disease was formerly known as atypical celiac disease.
Symptoms can be for example:
- Flatulence
- Indigestion
- Change in bowel habits (for example, diarrhea or constipation)
- Insomnia, tiredness
- Depressions
In some cases, the (slightly) symptomatic celiac disease is discovered by chance during the investigation of elevated liver values, low iron values or thyroid dysfunction. Gluten-free food clearly helps to ease the symptoms.
Subclinical form of celiac disease
These people do not show any signs of illness. However, the typical antibodies are found in the blood as well as celiac disease-specific changes in the small intestinal mucosa. A gluten-free diet is therefore still necessary. Most patients with subclinical celiac disease then find that they feel better without gluten, even though they had no previous symptoms.
Refractory celiac disease
In refractory type 2 celiac disease, the symptoms persist for at least a year or come back despite a strict gluten-free diet. As a rule, those affected are adults over the age of 50. These people should be examined and treated in a specialized centre, also because of the increased risk of a rare type of cancer in the intestine (intestinal T-cell lymphoma).
Refractory celiac disease type 1 can be distinguished by a greatly increased sensitivity to gluten. In classical medicine, it is treated successfully with drugs that are also used in patients with inflammatory bowel disease.
Potential celiac disease
This diagnosis is usually an incidental finding or the result of testing relatives of celiac patients. The people affected usually have little or no complaints. Corresponding antibodies can be detected in a gluten-containing diet, but no changes in the mucous membrane of the small intestine that are typical of celiac disease. Celiac disease may develop if the gluten exposure is higher. These people should therefore be monitored, and antibodies and findings in the small intestine mucosa should be checked regularly. If such changes develop, you should switch to a gluten-free diet.
Causes: where does celiac disease come from?
Various factors play a role in the development of celiac disease. In any case, two prerequisites must be met for a person to fall ill:
Prerequisite 1: genetic predisposition
A genetic predisposition, which occurs in 30 to 40 percent of the population, increases the risk of developing celiac disease three times. It concerns the presence of certain surface features on immune cells: the proteins HLA-DQ2 or HLA-DQ8. If they do not find each other, the doctor can rule out celiac disease.
Due to the genetic condition mentioned, there is a familial predisposition to celiac disease. If a first-degree relative (siblings, parents or children) has celiac disease, the family members are also at an increased risk (around 10 to 15 percent) of having or developing celiac disease.
Requirement 2: an autoimmune reaction
Gluten is not completely digested. Undigested fragments of the gluten molecules are taken up by the mucous membrane of the small intestine and can be presented by the immune cells of people with HLA-DQ2 or -DQ8 and incorrectly recognized as an “enemy” – similar to a pathogen causing a bacterial or viral infection. The activation of the immune system is even more pronounced when the gluten fragments react with the body’s own enzyme tissue transglutaminase (tTG), which occurs in the entire intestine. Defence substances, so-called antibodies, then also arise against this enzyme. Since these antibodies are directed against the body’s own tissue, one speaks of an autoimmune reaction or disease.
Other factors that can possibly promote the development of celiac disease are, for example, early and massive contact with gluten in genetically predisposed children or intestinal infections.
Diagnosis: How do you detect celiac disease?
What to do?
If you suspect celiac disease or if you have the symptoms mentioned above, it is best to first contact your GP or, if a baby or child is affected, the pediatrician. Both can run some initial tests and refer you to a gastroenterologist if necessary.
Alternatively, you can immediately go on a strict GF diet for 4 weeks. See if your symptoms improve. Then have a large portion of gluten foods (e.g. spaghetti) and see how your body reacts. Your body will usually tell you in no uncertain terms if it is happy with your food choice or not.
Antibody test
The detection of so-called autoantibodies against the enzyme tissue transglutaminase (tTG-IgA) in the blood provides a decisive first clue. They can be found in more than 97 percent of patients with active celiac disease, provided they have not been eating gluten-free for many months. More rarely, antibodies against the so-called endomysium (EMA-IgA) are determined, which have a similarly high informative value.
Antibodies against the gluten component gliadin (deaminated gliadin peptides, DGP-IgG) are the second choice and should only be used for the initial diagnosis of celiac disease if there is an IgA deficiency.
Important: The antibody test from the blood is only meaningful if the person concerned is not on a gluten-free diet or has only been on a gluten-free diet for a few weeks. Antibody levels normalize under gluten-free or very low-gluten foods. They fall within 30 to 50 days by half of the respective initial value and they are then soon no longer detectable.
At the same time, a total IgA value should always be determined in order to rule out an IgA deficiency that occurs in around three to seven percent of celiac disease patients. If there is an IgA deficiency, a negative test for tTG-IgA would not be meaningful. Instead of immunoglobulins A, immunoglobulins G should then be determined against tissue transglutaminase or against deamidated gliadin (IgG anti-DGP).
Biopsy
If the doctor has been able to detect antibodies, samples should be taken from the lining of the small intestine and examined for changes that are typical of celiac disease. This requires a reflection of the stomach and small intestine.
With the help of a special, tube-like device (endoscope), the doctor can view the inside of the stomach and upper small intestine during a gastroscopy. He can also take tissue samples (biopsies) from the mucous membrane of the small intestine, which are then examined under the microscope for the typical changes in celiac disease. The gastroscopy usually takes place on an outpatient basis, takes about ten minutes and is considered to be low-risk.
Using a tissue sample from the mucous membrane of the small intestine (small intestine biopsy), the changes in the mucous membrane typical of celiac disease can be seen under the microscope. It does not fold up into numerous protuberances, as it normally does, but these villi appear flattened or absent entirely. At the same time, pronounced crypts (deepening of the mucous membrane) and accumulations of lymphocytes (immune cells) within the mucous membrane can occur.
Do you always need a biopsy?
Children can sometimes do without a small intestine biopsy. If you
- have very high tTG antibody levels (more than ten times higher),
- multiple increased endomysial antibodies were detectable from different blood samples,
- the genetic testing revealed the presence of HLA-DQ2 or -DQ8 and
- the complaints under gluten-free diet disappear
you can be spared the gastroscopy, as the diagnosis can also be made that way.
What About Home Celiac Self-Tests?
Self-tests from pharmacies, the Internet or drugstores cannot diagnose celiac disease. For a simple reason: in the best case scenario – if done correctly – you will detect celiac disease-relevant antibodies in the blood. This can be an indication of celiac disease, but is not enough on its own for a diagnosis.
In adults, samples are generally still required to be taken from the mucous membrane of the small intestine, especially if the symptoms are only moderately pronounced. In children, at least a quantitative determination of antibodies and other positive blood values or the detection of HLA-DQ2 or HLA-DQ8 are necessary in order to make the diagnosis of celiac disease.
Because of its inaccuracy, a negative self-test does not definitely exclude celiac disease.
Therapy: how can celiac disease be treated?
Currently, the only way to treat celiac disease is to follow a strict gluten-free diet, which the patient must adhere to for the rest of their lives.
Even without gluten, a person can have such a balanced diet that they can consume sufficient quantities of all the important nutrients. If there are deficiencies, for example in iron, calcium, magnesium, vitamin B12, folic acid or vitamin D, then the patient should additionally supply the missing nutrients over a few weeks or even longer.
Some people with celiac disease have limited digestion of fat and lactose and therefore have additional problems such as diarrhea or flatulence. You may need to temporarily avoid fat and certain dairy products until the intestinal mucosa has recovered from the gluten-free diet.
How quickly does a gluten-free diet work?
In about two-thirds of patients, the symptoms improve in about two weeks with a gluten-free diet.
The changes in the intestinal mucosa also usually subside after a few months: the inflammation subsides and the villi, which are so important for nutrient absorption, develop again.
The risk of complications and long-term consequences drops to normal after a few years with a strictly gluten-free diet.
The risk of degeneration of the mucous membrane of the small intestine (intestinal lymphoma) also decreases rapidly with a strict gluten-free diet.
What does gluten-free diet mean?
Gluten-free food means that no products that contain gluten may be consumed. The adhesive protein gluten occurs in the following types of grain:
- wheat
- barley
- rye
- Spelt
- Khorasan wheat
- Emmer
- Bulgur (some varieties)
- triticale
- farina
- kamut
- farro
- couscous
Celiac sufferers should avoid these grains and products that contain them. If a product is declared gluten-free on the packaging, gluten must not be contained in an amount that could harm a celiac patient. The prescribed guideline value for gluten-free products in Australia is 200 parts per million or milligrams per kilogram. In other countries, it is as low as 20 ppm.
Gluten-free include:
- Corn
- rice
- millet
- Buckwheat
- soy
- sesame
- Potatoes
- Quinoa
- amaranth
Oats are inherently gluten-free but are often contaminated with gluten during normal harvest and processing. Therefore, celiac patients should only use oats that have been declared gluten-free due to the manufacturing process.
Important: Even if the intestinal disease is mild or allegedly symptom-free, the patient should strictly avoid gluten. Otherwise, the inflammation in the intestinal mucosa continues – with the risk of long-term complications, such as a nutritional deficiency with its consequences such as short stature, osteoporosis or reduced performance, or in the worst case, the development of the above-mentioned small intestinal cancer (intestinal lymphoma, adenocarcinoma)
Co-morbidities
Celiac disease often occurs together with other diseases. This has to do with the underlying genetic makeup. The presence of HLA-DQ2 and/or HLA-DQ8 on the immune cells also favours other autoimmune diseases. The continued consumption of gluten can increase the risk of autoimmune diseases that often occur in combination with celiac disease.
The diseases that often coexist with celiac disease include, among others
- Type 1 diabetes mellitus
- Autoimmune diseases of the thyroid gland ( Hashimoto’s thyroiditis, Graves’ disease)
- Autoimmune diseases of the skin (dermatitis herpetiformis)
- Autoimmune hepatitis
- Primary biliary cirrhosis
- a certain type of hair loss ( alopecia areata )
- Psoriasis
- Rheumatoid arthritis
- other rheumatic diseases.
Celiac disease often occurs in other genetic diseases (Down syndrome, Turner syndrome).
We are all GF at the Vitalis Colon Wellbeing centre and are happy to support you in this journey.




0 Comments